Pre-emptive pharmacogenetics integrated into EHR enables personalised prescribing decisions
Science to Practice Latest highlights on drug safety and efficacy
16.4.2026
Pharmacogenomics (PGx) can clarify why individuals respond differently to medications and why some experience adverse drug reactions. Although clinical guidelines such as those from CPIC (U.S.) and DPWG (Dutch) provide recommendations for genotype- or phenotype-informed prescribing, putting these frameworks into routine care is still difficult. Key barriers include standardised communication of results and integration of information into electronic health record (EHR) systems.
The value of pharmacogenomics lies in its ability to translate genetic insight into actionable prescribing decisions. Integrated into clinical workflows, it enables safer and more individualised treatment.
In a cohort of 255 patients, nearly all (95%) carried at least one variant associated with an actionable (according to CPIC/DPWG guidelines) gene variant. The most frequently affected medications included statins, 5-fluorouracil, irinotecan, and pantoprazole. Clinically relevant PGx-based guidance was issued for 21.5% of patients, and in three quarters of these cases (75.5%) hospital physicians adjusted therapy accordingly.
The program also detected 57 clinically significant drug–drug interactions, with pharmacogenetically relevant drugs involved in about one fifth (21%) of cases. Following discharge, general practitioners continued the optimised regimen in 77% of patients whose medication was changed during hospitalisation. Around 10% of patients discussed their PGx results with their general practitioner. General practitioners expressed positive attitudes toward using PGx in future prescribing while highlighting the need for additional training.
Overall, the findings suggest that proactive PGx testing can be integrated successfully into hospital care, is well received by both hospital clinicians and general practitioners, and that embedding results in the EHR is a practical strategy to support wider uptake of precision prescribing (1).
Explore Medbase’s dedicated pharmacogenetic database, Pgxbase, for more information on the impact of genetic variants on drug safety and efficacy.
News produced by Medbase Medical Team
References
Tremmel R, Schreeck F, Jaeger S, Schricker S, Schaeffeler E, Igel S, Steinberger D, Pagitz M, Latus J, Ketteler M, Bühl K, Dahlke MH, Kopp HG, Schwab M. Clinical Implementation of Pharmacogenomics and Drug-Drug Interaction Screening in a German Academic Teaching Hospital and Outpatient Follow-Up. Clin Pharmacol Ther. 2026 Jan;119(1):241-254. doi: 10.1002/cpt.70083. Epub 2025 Oct 11. PMID: 41074844; PMCID: PMC12746526.
Preventing drug-related problems in CKD – medication review shows major clinical and economic benefits
Science to Practice Latest highlights on drug safety and efficacy
30.3.2026
Patients with chronic kidney disease (CKD) are particularly prone to drug-related problems due to polypharmacy and the need for dose adjustments and monitoring.
In a prospective study of 142 hospitalised CKD patients, clinical pharmacist-led medication reconciliation combined with medication review produced substantial economic benefits. Over a four-month period, preventing and resolving medication discrepancies and other drug-related problems generated an estimated net benefit of USD 81 871 (USD 577 per patient) and a benefit-to-cost ratio of 115.7:1.
These results highlight the clinical and economic value of systematic medication review in high-risk patients. As manual review is resource-intensive, clinical decision support systems that automatically flag potential drug-related problems could help clinicians and pharmacists apply these safety principles more consistently in everyday practice.
The value of medication review in CKD lies in prevention: improving patient safety while reducing healthcare costs.
For more comprehensive information, explore Renbase, our specialised database that provides detailed insights on drug safety and efficacy when treating patients with renal failure.
News produced by Medbase Medical Team
References
Altawalbeh SM, Sallam NM, Al-Khatib M, et al. Clinical pharmacist-led medication reconciliation supplemented with medication review in admitted patients with chronic kidney disease: a cost-benefit analysis. BMJ Open. 2025;15:e087232. doi:10.1136/bmjopen-2024-087232. PMID: 40322147.
Bored of drug interaction alerts? One size doesn’t fit all!
Optimising alert accuracy, clinical relevance, and patient-specific integration is essential
Science to Practice Latest highlights on drug safety and efficacy
10.3.2026
Electronic drug–drug interaction (DDI) alerts are a core component of medication safety. A 2025 systematic review (8 studies; N=43,413) found that DDI alerts increase targeted clinician actions, such as modifying prescriptions or ordering monitoring tests (OR 2.08; 95% CI 1.01–4.27). Effects were strongest when alerts were clearly actionable and clinically relevant (1).
While evidence for downstream patient outcomes remains limited, the review provides important insight into why: many systems relied on broad, non–patient-specific rules and generated high alert volumes (1).
How to maximise clinical relevance while minimising burden:
Prioritise high-risk DDIs (e.g., serious, well-established interactions) rather than alerting on theoretical combinations
Integrate patient-specific context (labs, renal function, comorbidities, current doses) to improve clinical relevance
Design actionable alerts with clear next steps (dose adjustment, monitoring recommendation, alternative drug)
Avoid unnecessary “hard stops”; use interruptive alerts selectively for highest-risk scenarios
Measure performance locally: track override patterns, monitoring completion, and incidence of preventable DDI-related harm
Drug–drug interaction decision support can improve patients’ outcomes. The path to do so lies in precision, relevance, and continuous optimization of alert design. Don’t settle for less.
The value of drug–drug interaction decision support lies in precision: delivering the right alert, for the right patient, at the right moment. Clinically relevant, patient-specific alerts support safer prescribing while minimising alert fatigue.
For more comprehensive information, explore Inxbase, our specialised database that provides detailed descriptions of each interaction, along with practical guidance on how to avoid or manage the associated clinical risks.
News produced by Medbase Medical Team
References
Holbrook AM, Matos Silva J, Faruque JAY, et al. Effect of electronic drug-drug interaction alerts on patient and clinician outcomes: a systematic review. J Am Med Inform Assoc. 2025;32(10):1617–1628.
Topical retinoids are not likely to increase risk of major congenital malformations
Science to Practice Latest highlights on drug safety and efficacy
18.2.2026
Due to high risk of teratogenicity, systemic use of retinoids is strictly forbidden for women of reproductive potential not using efficient method(s) of contraception. There are specific measures to prevent inadvertent pregnancies, like regular monthly pregnancy tests for the users of systemic isotretinoin, and limiting the right to prescribe of isotretinoin to only dermatologists, and restricting the length of validity for prescriptions.
Based on teratogenicity of isotretinoin, also the use of topical retinoids like adapalene for the treatment of acne should be avoided in women of childbearing potential. Large-scale, population-based data on the use of topical retinoids has been lacking, however.
A large Nordic cohort study finds no increased risk of major congenital malformations with first-trimester exposure to topical retinoids – although precautionary use in pregnancy remains justified.
In a recent population-based cohort study from Denmark, Iceland, Norway, and Sweden, use of topical retinoids increased over 3-fold over the 18-year study period (2006-2024). Of the almost 3.9 million infants included in the cohort, 0.86 per 1000 were exposed to topical retinoids during the first trimester. There was no increase in risk for major congenital malformations when comparing the exposed to unexposed, or to infants exposed to azelaic acid or clindamycin. Among the 2172 infants exposed to topical retinoids, 71 had any major congenital malformation (3.3%) (1).
There are important limitations in the study, however. Most importantly, there is a possibility of underestimation of the frequency of use and the risk of congenital malformations due to exclusion of pregnancies that ended before 22 weeks of gestation. The authors concluded that a safety precaution for use in pregnancy is still justified, but findings of the study could provide reassurance for women who become pregnant while using topical retinoids (1).
For more comprehensive information, explore Gravbase and Lactbase, our specialised databases providing detailed insights on drug safety and efficacy during pregnancy and lactation.
News produced by Medbase Medical Team
References
Refsum E, Furu K, Cesta CE, Nørgaard M, Wittström F, Zoega H, Ulrichsen SP, Cohen JM. Topical retinoid use in women of reproductive age and risk of major congenital malformations in exposed pregnancies – a Nordic cohort study. Br J Dermatol. 2025 Dec.
Paracetamol is still the safest drug to treat pain and fever during pregnancy
Science to Practice Latest highlights on drug safety and efficacy
29.10.2025
There is an ongoing public and global debate about possible adverse developmental long-term effects of maternal use of paracetamol during pregnancy. During the last years, research has been focusing on allergic and neurodevelopmental outcomes in the infants exposed to paracetamol via maternal use, and these themes are obviously reflected in the mainstream media and discussions in social media, as well as among professionals.
Our medical team at Medbase has been following the accumulation of novel studies and clinical evidence of safety of medications, including paracetamol, for 18 years now. Up to date, we have included over 60 relevant references for original research on paracetamol use during pregnancy, and based on these data, given a clinically useful interpretation based only on rigorous scientific work.
Based on this very solid evidence, our Gravbase recommendation – part of Medbase’s clinical decision support on drug safety in pregnancy – confirms that paracetamol remains the preferred option for pain management during pregnancy, given that indication is clear, the need for long-term use is thoroughly assessed, and recommended daily doses are followed.
Eighteen years of clinical evidence still point to one conclusion: paracetamol remains the most reliable option when used as recommended.
In a recent article in the British Medical Journal, Dr Jeffrey K Aronson from the Centre for Evidence Based Medicine, Oxford, UK, discusses elegantly the importance of random discoveries in drug development and confounding factors in epidemiological studies on paracetamol, in which relatively vague associations with e.g. asthmatic outcomes and adverse neurodevelopmental outcomes, including ADHD and autism, have been suggested already since 2013. He especially acknowledges confounding by indication and other biases, like the use of antibiotics as well as viral infections in childhood and recall bias in questionnaire studies (1).
Confounders like household factors and environment can be partially overcome with sibling control analysis that was deployed also in a nationwide Swedish study with over 185 000 pregnancy exposures to paracetamol. The clinically likely unmeaningfully small 5% increase, leading to 0.09% difference in risk for autism at 10 years of age disappeared completely in the matched sibling-controlled analyses, highlighting the impact of shared genetic background and childhood environment on neurodevelopment (2).
For more comprehensive information, explore Gravbase and Lactbase, our specialised databases providing detailed insights on drug safety and efficacy during pregnancy and lactation.
Ahlqvist VH, Sjöqvist H, Dalman C, Karlsson H, Stephansson O, Johansson S, Magnusson C, Gardner RM, Lee BK. Acetaminophen Use During Pregnancy and Children’s Risk of Autism, ADHD, and Intellectual Disability. JAMA. 2024 Apr 9;331(14):1205-1214. https://pubmed.ncbi.nlm.nih.gov/38592388/
Science to Practice Latest highlights on drug safety and efficacy
9.9.2025
Older adults face high risks of medication errors and adverse drug events due to polypharmacy and age-related changes. A new systematic review examined 16 randomised controlled trials with over 135,000 participants.
Clinical decision support systems (CDSS) reduced the initiation of potentially inappropriate medications by up to 18% (1). CDSS interventions increased deprescribing rates, with 55% of older patients discontinuing inappropriate drugs, compared to 30% in control groups (2).
CDSS enables safer prescribing for older adults by reducing inappropriate drugs and supporting deprescribing. Success depends on clinician engagement, smart alerts, and workflow integration.
What it means for clinical practice: CDSS can support safer prescribing, but success depends on clinician engagement, system usability, and reducing low-importance alerts to avoid alert fatigue. Collaboration with pharmacists and integration into clinical workflows are key to achieving meaningful outcomes.
Takeaway: CDSS are promising tools to optimise prescribing for older adults, provided that their contents are evidence-based and cover all relevant areas of drug treatment. In addition to technology, human factors, training, and system design determine whether safety gains translate into real-world impact.
Discover Medbase Knowledgebase, our trusted, comprehensive source of drug safety and efficacy information across all clinically relevant areas of pharmacotherapy.
News produced by Medbase Medical Team
References
Ng Y, Hsu JTY, Ng NNE, Ong JZE, Hsu JLJ, Sulaimi F, Tan HK, Tang ASP, Ng QX. Evaluating the role of clinical decision support systems in medication safety for older people: a systematic review. Age Ageing. 2025 Jul 1;54(7):afaf206. doi: 10.1093/ageing/afaf206. PMID: 40716041; PMCID: PMC12296344.
McDonald EG, Wu PE, Rashidi B et al. The MedSafer study—Electronic decision support for deprescribing in hospitalized older adults: A cluster randomized clinical trial. JAMA Intern Med. 2022;182:265–73. https://doi.org/10.1001/jamainternmed.2021.7429.
Inter-compound variability in drug-induced liver injury: a neglected factor in safety assessment
Science to Practice Latest highlights on drug safety and efficacy
26.9.2025
Idiosyncratic drug-induced liver injury (DILI), though uncommon, remains the leading cause of drug withdrawals from the market and the second most common cause of acute liver failure (following paracetamol overdose). Despite its clinical significance, DILI risk is still frequently overlooked at the time of drug initiation and is rarely evaluated on a compound-specific level.
The U.S. DILI Network (DILIN) has helped to quantify individual drug risk by estimating real-world DILI incidences (1). In their prospective cohort study, azathioprine showed the highest estimated incidence – approximately 1 in 350 prescriptions – underscoring the need for improved safety stratification in commonly used drugs (1). Other well-documented agents include amoxicillin-clavulanate, isoniazid, diclofenac, and flucloxacillin, all of which demonstrate variability in both injury pattern and clinical presentation. Additionally, older antiepileptic drugs were a major contributor to hepatotoxicity risk. Notably valproic acid, phenytoin, carbamazepine, lamotrigine and phenobarbital (1).
Not all drugs carry the same liver risk. Drug-induced liver injury (DILI) is the leading cause of drug withdrawals – yet safety assessments still generalise across classes. A tailored, compound-specific approach is essential for safer prescribing and regulatory alignment.
Despite clear evidence of inter-compound differences, many prescribing practices and safety communications still generalize DILI risk across drug classes. A more tailored approach – one that incorporates relevant pharmacologic properties, and real-world incidence – is essential for safer prescribing and better regulatory alignment.
For more comprehensive information, explore Heparbase, our specialised database providing detailed insights on drug safety and efficacy when treating patients with hepatic impairment.
News produced by Medbase Medical Team
References
Chen VL, Rockey DC, Bjornsson ES, Barnhart H, Hoofnagle JH, for the Drug-Induced Liver Injury Network Investigators. Incidence of Idiosyncratic DrugInduced Liver Injury Caused by Prescription Drugs.Drug Saf. 2025;48(2):151–160. PMID: 39317916. doi:10.1007/s40264-024-01486-6
Inhaled beta-sympathomimetics should be continued during pregnancy
Science to Practice Latest highlights on drug safety and efficacy
1.7.2025
In the treatment of asthma during pregnancy, the primary focus should be on effective asthma control, as poorly controlled asthma poses a greater risk to pregnancy than most asthma medications, especially inhaled medications used at normal doses.
Based on available clinical data and animal studies, inhaled beta-sympathomimetics do not cause malformations nor have toxic effects on the foetus or newborn. The use of systemic beta-sympathomimetics during pregnancy may cause transient tachycardia in both the foetus and the mother, but this is considered harmless. Decreases in blood pressure and transient hyperglycaemia have also been reported. Use of beta-sympathomimetics in late pregnancy may reduce uterine contractions and prolong labour. There are rarely clinical indications for systemic use of asthma medications during pregnancy, however (1).
Maintaining asthma control during pregnancy is essential for maternal and foetal wellbeing. Inhaled beta-sympathomimetics are considered safe and should not be discontinued unnecessarily.
Of these drugs, most human pregnancy data is gathered from exposures to salmeterol and formoterol, while for indacaterol and vilanterol there are no published human exposure data available so far. However, maternal and foetal risks related to uncontrolled asthma during pregnancy outweigh any theoretical harm associated with any of these drugs.
To avoid inappropriate pausing or tapering of effective asthma medications due to unjustified concerns related to pregnancy, we have updated and harmonised the Gravbase recommendation texts and classifications for the inhaled beta-sympathomimetics formoterol, salmeterol, indacaterol and vilanterol. Please see the detailed and referenced background information from our Knowledgebase -documents. Any feedback is welcomed as well as an integral part of improving our products.
For more comprehensive information, explore Gravbase and Lactbase, our specialised databases providing detailed insights on drug safety and efficacy during pregnancy and lactation.
News produced by Medbase Medical Team
References
Jones CE, Jamil Y. Management of asthma in pregnancy. Clin Med (Lond). 2025 Jan;25(1):100277. doi: 10.1016/j.clinme.2024.100277. Epub 2024 Dec 17. PMID: 39701495; PMCID: PMC11773012.
Severe drug interactions challenge COVID-19 Treatment – nirmatrelvir/ritonavir and tacrolimus require special attention
Science to Practice Latest highlights on drug safety and efficacy
18.6.2025
Nirmatrelvir/ritonavir, NMV/r (PAXLOVID™) is first oral antiviral for COVID-19. However, it poses significant risks for drug interactions, particularly for patients on immunosuppressive therapy such as tacrolimus. Ritonavir strongly inhibits CYP3A4 and P-glycoprotein, leading to dangerous increases in the levels of several co-administered drugs (1,2,3).
A real-world study from London found that nearly 90% of patients treated with NMV/r had potential drug-drug interactions, and 8% had to forgo treatment due to risk, and 53% required management. Alarmingly, more than half of the cases requiring intervention lacked documented guidance in EHR (4).
Up to 90% of patients treated with NMV/r face potential drug interactions – and over half of those requiring intervention lacked documented guidance in EHRs.
Numerous case reports have highlighted severe tacrolimus toxicity in transplant recipients treated with NMV/r. Based on this, clinical recommendations advise a substantial dose reduction or treatment interruption to maintain therapeutic whole blood levels if ritonavir is co-administered with tacrolimus. This adjustment should be guided by an experienced physician, in settings where daily tacrolimus monitoring is feasible (5,6,7,8,9,10).
Ultimately, NMV/r treatment requires individualized medication management and close monitoring—particularly in immunocompromised patients. Clinical pharmacology support is essential to ensure safety, avoid toxicity, and provide effective care in complex therapeutic situations.
For comprehensive insights into drug-drug interactions and adverse drug reactions, explore our databases Inxbase and Riskbase.
News produced by Medbase Medical Team
References
Stoiber A, Gray G, Sailer G, Huf W, Tonna A. Frequency, type and severity of drug-related problems and pharmacist interventions in Paxlovid® prescribing: a descriptive analysis. Int J Clin Pharm. 2025 Apr;47(2):471-476. PMID: 39708268
Mozaffari E, Chandak A, Ustianowski A, Rivera CG, Ahuja N, Jiang H, Berry M, Okulicz JF, Amin AN. Prevalence of Potential Drug Interactions With Direct-Acting Antivirals for COVID-19 Among Hospitalized Patients. Clin Ther. 2024 Oct;46(10):778-784. PMID: 39244489
Gerhart J, Cox DS, Singh RSP, Chan PLS, Rao R, Allen R, Shi H, Masters JC, Damle B. A Comprehensive Review of the Clinical Pharmacokinetics, Pharmacodynamics, and Drug Interactions of Nirmatrelvir/Ritonavir. Clin Pharmacokinet. 2024 Jan;63(1):27-42. PMID: 38177893
Bukhari S, Hughes S, Mughal N, Moore LSP, Davies G, Vargas Zhang A, Ng M, Karagozlu Z, Boffito M. Nirmatrelvir/ritonavir: real world drug-drug interaction management experience. Expert Rev Anti Infect Ther. 2024 Sep;22(9):781-783. PMID: 39109469
Sabo AN, Cunat S, Kemmel V. Delayed Drug-Drug Interaction Between Antiviral Drugs and Tacrolimus in a Pancreatic Islet Transplant Recipient with SARS-CoV-2 Pneumonia-A Case Study. Ther Drug Monit. 2025 Feb 3; PMID: 39898493
Lipsitz J, Chowdary AR, Tsai P, Quigley R. Paxlovid-induced tacrolimus toxicity in a 16-year-old male with steroid-resistant nephrotic syndrome. Pediatr Nephrol. 2025 Feb 25; PMID: 39998631
Schneider J, Wobser R, Kühn W, Wagner D, Tanriver Y, Walz G. Nirmatrelvir/ritonavir treatment in SARS-CoV-2 positive kidney transplant recipients – a case series with four patients. BMC Nephrol. 2023 Apr 15;24(1):99 PMID: 37061677
Lemaitre F, Budde K, Van Gelder T, Bergan S, Lawson R, Noceti O, Venkataramanan R, Elens L, Moes DJAR, Hesselink DA, Pawinski T, Johnson-Davis KL, De Winter BCM, Pattanaik S, Brunet M, Masuda S, Langman LJ. Therapeutic Drug Monitoring and Dosage Adjustments of Immunosuppressive Drugs When Combined With Nirmatrelvir/Ritonavir in Patients With COVID-19. Ther Drug Monit. 2023 Apr 1;45(2):191-199 PMID: 35944126
Dewey KW, Yen B, Lazo J, Seijo L, Jariwala R, Shah RJ, Quan D, Carpenter B, Paul Singer J, Breen K, Hays S, Florez R. Nirmatrelvir/ritonavir Use With Tacrolimus in Lung Transplant Recipients: A Single-center Case Series. Transplantation. 2023 May 1;107(5):1200-1205 PMID: 3652555
Giguère P, Deschenes MJ, Loon MV, Hoar S, Fairhead T, Pazhekattu R, Knoll G, Karpinski J, Parikh N, McDougall J, McGuinty M, Hiremath S. Management and Outcome of COVID-19 Infection Using Nirmatrelvir/Ritonavir in Kidney Transplant Patients. Clin J Am Soc Nephrol. 2023 Apr 26;18(7):913-9 PMID: 37099447.
NSAIDs to be avoided during the second half of pregnancy
Science to Practice Latest highlights on drug safety and efficacy
2.6.2025
Drug authorities in the EU, UK and USA have set stricter warnings concerning the use of non-steroidal anti-inflammatory drugs (NSAIDs) in pregnancy, pointing out increased risk for oligohydramnios and premature closure of ductus arteriosus with the use of NSAIDs from mid-pregnancy (gestational week 20) onwards (1).
Following these warnings and a study from the German Embryotox cohort (2), the manufacturers have updated the European summaries of product characteristics (SPCs) to include this warning as well as a contra-indication for the systemic use of these drugs during the third trimester of pregnancy. The use of NSAIDs during the third trimester may also prolong bleeding time in both mother and child, as well as lead to delayed or prolonged labor.
NSAIDs should be avoided from mid-pregnancy onwards due to increased risks for the fetus. Gravbase classification has been updated accordingly to ensure safer drug use during pregnancy.
Our recommendations in Gravbase have been updated accordingly, and the classification of these drugs has been uniformly changed to C2. Occasional use, especially during the first half of pregnancy, appears relatively safe.
For more comprehensive information, explore Gravbase and Lactbase, our specialised databases providing detailed insights on drug safety and efficacy during pregnancy and lactation.
News produced by Medbase Medical Team
References
FDA recommends avoiding use of NSAIDs in pregnancy at 20 weeks or later because they can result in low amniotic fluid. 10-15-2020 FDA Drug Safety Communication.
Dathe, K., Frank, J., Padberg, S. et al. Fetal adverse effects following NSAID or metamizole exposure in the 2nd and 3rd trimester: an evaluation of the German Embryotox cohort. BMC Pregnancy Childbirth 22, 666 (2022) https://pubmed.ncbi.nlm.nih.gov/36028798/
False penicillin allergy labels are common – but solutions exist
Science to Practice Latest highlights on drug safety and efficacy
28.4.2025
According to recent research, over 95% of people labeled as allergic to penicillin are not truly allergic. Nevertheless, millions of patients continue to avoid β-lactam antibiotics, leading to the use of less effective alternatives, increased antibiotic resistance, and higher healthcare costs (1).
In the United States, 10–15% of hospitalised patients carry a penicillin allergy label, whereas in parts of Europe the figure is below 3%. However, true IgE-mediated allergy is confirmed in only 1–2% of cases. Direct drug provocation testing (DPT) has proven to be a safe, fast, and cost-effective method for removing incorrect allergy labels, especially in low-risk patients (1).
Over 95% of penicillin allergy labels are incorrect – yet millions still avoid effective treatments. Safe and simple testing can restore access to first-line antibiotics, reduce resistance, and lower healthcare costs.
Meta-analyses show that over 94% of patients tolerate penicillin after testing, with adverse reactions —mostly mild – occurring in less than 2% of cases. Non-allergist physicians and healthcare professionals are increasingly involved in delabeling, supported by validated tools and guidelines (1).
Despite promising results, fewer than 40% of eligible patients undergo delabeling. Integrating delabeling into antibiotic stewardship and treatment protocols is particularly important in countries with limited access to allergists (1). In addition, a verified penicillin allergy should be documented at the individual drug level (e.g. amoxicillin), as cross-reactivity varies between different penicillins and other beta-lactam antibiotics (2,3).
Healthcare systems should develop scalable and efficient strategies to address this widespread issue.
For more comprehensive insights, explore Xreactbase, our specialised database designed to identify potential drug cross-hypersensitivities.
News produced by Medbase Medical Team
References
Tejedor-Alonso MA, Perez-Encinas M, Sanz Márquez S, Martinez Simon JJ, Moreno-Nuñez L, Gonzalez-Moreno A, Macias-Iglesias J, Rosado-Ingelmo A. How Far Are We From Achieving Delabeling of False Penicillin/ß-Lactam Allergy Alerts? A Population Problem. J Investig Allergol Clin Immunol. 2025 Feb 18;35(1):12-23. https://pubmed.ncbi.nlm.nih.gov/38725322/
Romano A, Atanaskovic-Markovic M, Barbaud A, Bircher AJ, Brockow K, Caubet JC, Celik G, Cernadas J, Chiriac AM, Demoly P, Garvey LH, Mayorga C, Nakonechna A, Whitaker P, Torres MJ. Towards a more precise diagnosis of hypersensitivity to beta-lactams – an EAACI position paper. Allergy. 2020 Jun;75(6):1300-1315.
Hutten EM, Bulatović Ćalasan M, Trubiano JA, Pleijhuis RG, Terreehorst I. Discrepancies in Beta-Lactam Antibiotics Cross-Reactivity: Implications for Clinical Practice. Allergy. 2025 Feb 21;
Semaglutide (Ozempic) use during breastfeeding – concerns related to rapid weight loss, not the drug itself
Science to practice Latest highlights on drug safety and efficacy
1.4.2025
Semaglutide (Ozempic) is a glugacon-like peptide-1 (GLP-1) analogue, indicated for treatment of type 2 diabetes, and increasingly used for treating obesity. While little is known about its safety during breastfeeding, the large protein structure of semaglutide suggests that is unlikely to be excreted into breast milk in significant amounts, and the possible low amounts of semaglutide would be destroyed in the infant’s gastrointestinal tract prior to absorption.
Accordingly, semaglutide was not detected in breastmilk in a new study analysing milk samples from eight breastfeeding women who initiated semaglutide treatment (1). Infant development and growth were reported to be normal.
Semaglutide is unlikely to enter breast milk and was not detected in a recent study. However, rapid maternal weight loss may affect milk production and composition.
However, the authors raised concerns regarding maternal nutrient depletion due to rapid weight loss, which could potentially impact milk production and composition. The long-term effects on infants, particularly with early post-partum or chronic maternal use of higher doses of semaglutide, remain unknown.
For more comprehensive information, explore Gravbase and Lactbase, our specialised databases providing detailed insights on drug safety and efficacy during pregnancy and lactation.
News produced by Medbase Medical Team
References
Diab H, Fuquay T, Datta P, Bickel U, Thompson J, Krutsch K. Subcutaneous Semaglutide during Breastfeeding: Infant Safety Regarding Drug Transfer into Human Milk. Nutrients. 2024 Aug 28;16(17):2886.
Science to practice Latest highlights on drug safety and efficacy
17.2.2025
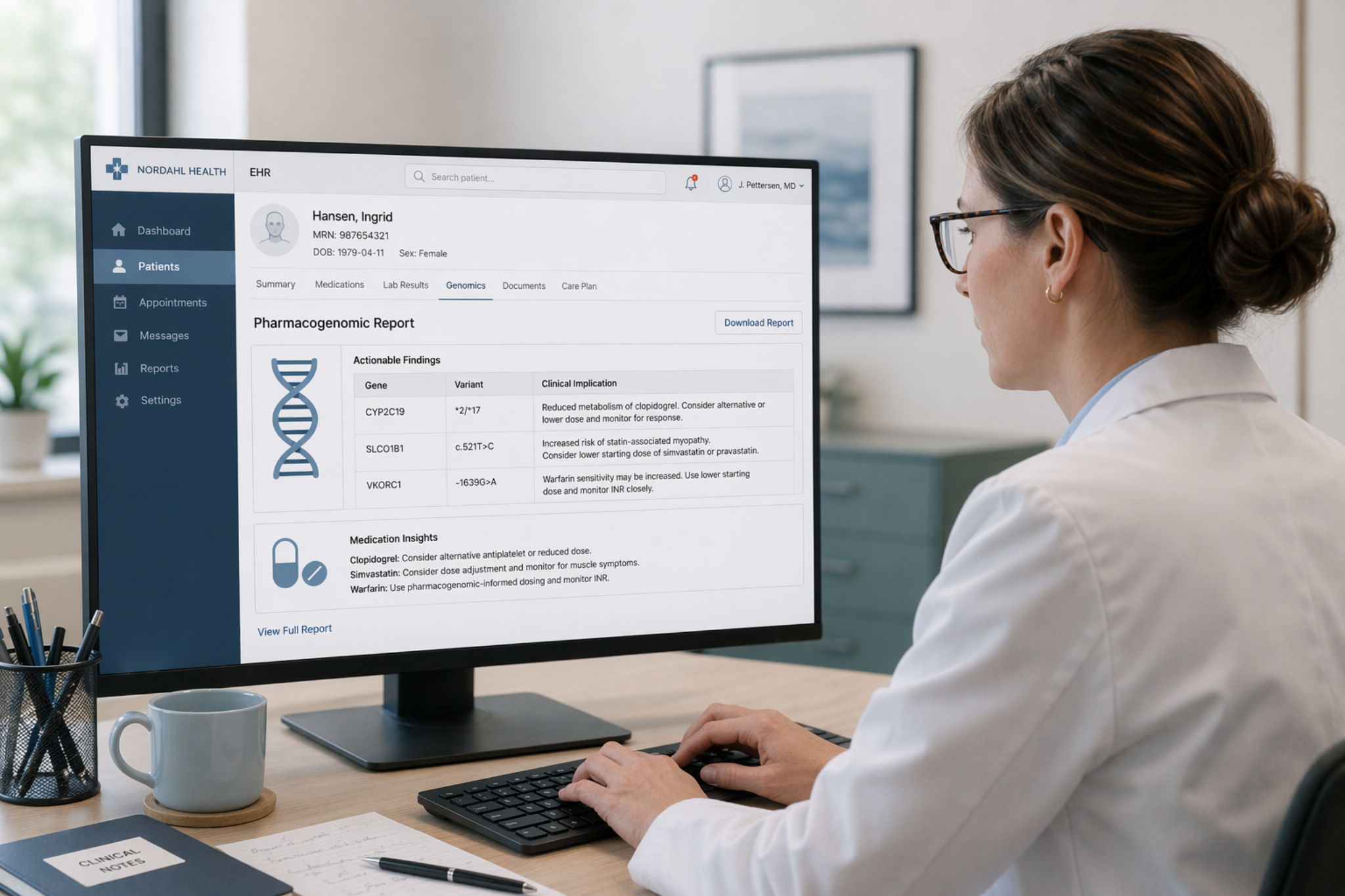
Patients who are compliant with their prescribed medication regimen may still exhibit significant variability in drug response, ranging from life-threatening adverse effects to complete lack of efficacy. This inter-individual variability is influenced by multiple factors, including co-medications that cause drug-drug interactions, liver and kidney function, age, gender, weight, and genetic variability (1).
Genetic variability plays a significant role in the pharmacokinetics of many cardiovascular drugs, where genes such as CYP2C9, CYP2C19, VKORC1, and SLCO1B1 affect the metabolism and efficacy of widely used medications like warfarin, clopidogrel, and statins (1). To mitigate the risks associated with drug use, computerised decision support systems (CDSS) have been developed to integrate patient-specific information into drug treatment recommendations (2).
Even patients who follow their prescribed medication regimen may experience vastly different drug responses, from life-threatening adverse effects to complete lack of efficacy.
Patients with a loss-of-function CYP2C19 allele may not efficiently metabolise clopidogrel to the active metabolite, leading to inadequate platelet inhibition and increased cardiovascular risk (3). Similarly, individuals with SLCO1B1 polymorphisms may experience statin-induced myopathy due to impaired hepatic uptake (4). While pharmacogenetics-driven precision medicine shows promise in studies, clinical decision support systems are needed to facilitate the implementation of pharmacogenetics and personalised drug treatment into everyday clinical practice.
Explore Medbase Knowledgebase for comprehensive insights on drug interactions, adverse effects, alternative drug and dosing recommendations, and more!
News produced by Medbase Medical Team
References
Ingelman-Sundberg M, Pirmohamed M. Precision medicine in cardiovascular therapeutics: Evaluating the role of pharmacogenetic analysis prior to drug treatment. J Intern Med. 2024 May;295(5):583-598. doi: 10.1111/joim.13772. Epub 2024 Feb 11. PMID: 38343077.
Bakker T, Klopotowska JE, Dongelmans DA, et al. The effect of computerised decision support alerts tailored to intensive care on the administration of high-risk drug combinations, and their monitoring: a cluster randomised stepped-wedge trial. Lancet. 2024 Feb 3;403(10425):439-449. doi: 10.1016/S0140-6736(23)02465-0. Epub 2024 Jan 20. PMID: 38262430.
Lee CR, Luzum JA, Sangkuhl K, Gammal RS, Sabatine MS, Stein CM, Kisor DF, Limdi NA, Lee YM, Scott SA, Hulot JS, Roden DM, Gaedigk A, Caudle KE, Klein TE, Johnson JA, Shuldiner AR. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2C19 Genotype and Clopidogrel Therapy: 2022 Update. Clin Pharmacol Ther. 2022 Nov;112(5):959-967
Cooper-DeHoff RM, Niemi M, Ramsey LB, Luzum JA, Tarkiainen EK, Straka RJ, Gong L, Tuteja S, Wilke RA, Wadelius M, Larson EA, Roden DM, Klein TE, Yee SW, Krauss RM, Turner RM, Palaniappan L, Gaedigk A, Giacomini KM, Caudle KE, Voora D. The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and Statin-Associated Musculoskeletal Symptoms. Clin Pharmacol Ther. 2022 May;111(5):1007-1021
Increased risk of hospitalisation due to drug interactions in older adults
Science to practice Latest highlights on drug safety and efficacy
31.1.2025
Clinically significant drug-drug interactions (DDIs) causing adverse drug events are common among older adults (1). A recent study found that these DDIs have a notable impact on the likelihood of hospital admissions related to adverse drug reactions (2).
This risk was particularly high for patients taking medications that increase the risk of bleeding, which doubled the likelihood of ADR-related admissions (2).
Notably, patients experiencing these DDIs also had lower health-related quality of life and extended hospital stays (1,2). These findings underscore the need for careful medication management in older adults.
Drug interactions in older adults can lead to serious adverse events, longer hospital stays, and reduced quality of life.
For comprehensive insights into drug-drug interactions and adverse drug reactions, explore our databases Inxbase and Riskbase.
News produced by Medbase Medical Team
References
Hughes JE, Bennett KE, Cahir C. Drug-Drug Interactions and Their Association with Adverse Health Outcomes in the Older Community-Dwelling Population: A Prospective Cohort Study. Clin Drug Investig. 2024 Jun;44(6):439-453. PMID: 38878216
Hughes JE, Moriarty F, Bennett KE, Cahir C. Drug-drug interactions and the risk of adverse drug reaction-related hospital admissions in the older population. Br J Clin Pharmacol. 2024 Apr;90(4):959-975. PMID: 37984336
Valproic acid and reproductive risks – the full story has not yet been told
Science to practice Latest highlights on drug safety and efficacy
22.1.2025
Valproic acid is a well-known teratogen, and maternal valproic acid use during pregnancy is associated with long-term offspring neurodevelopmental disorders and cognitive disturbances. The manufacturer also warns about male infertility. Lately, concerns have been raised by drug authorities in the EU and UK regarding possibility of paternally mediated disturbances of neurodevelopment.
However, in a large Danish registry study, there was no association of paternal pre-conception use of valproate with offspring risk of congenital malformations or neurodevelopmental disorders (1). Furthermore, a recent systematic review did not find any clear evidence for adverse effects of paternal exposure to antiseizure medications, including valproic acid, on offspring outcomes. The authors conclude that there is no justification for major concerns (2).
Recent research indicates no evidence linking paternal valproic acid use before conception to increased risks of congenital malformations or neurodevelopmental disorders in offspring.
For comprehensive insights into drug safety and efficacy during pregnancy and lactation, explore our databases Gravbase and Lactbase.
News produced by Medbase Medical Team
References
Christensen J, Trabjerg BB, Dreier JW. Valproate Use During Spermatogenesis and Risk to Offspring. JAMA Netw Open. 2024 Jun 3;7(6):e2414709. PMID: 38833248
Honybun E, Rayner G, Malpas CB, O’Brien TJ, Vajda FJ, Perucca P, Perucca E. Paternal exposure to antiseizure medications and offspring outcomes: a systematic review. J Neurol Neurosurg Psychiatry. 2024 Dec 16;96(1):15-25. PMID: 39299778.
All hope is not lost – tackling the global kidney disease burden with new therapeutics
Science to practice Latest highlights on drug safety and efficacy
8.1.2025
Kidney diseases now affect over 850 million people worldwide, and the numbers are steadily increasing, driven in part by the rising prevalence of diabetes. This growing burden places significant strain on healthcare systems globally (1).
Despite the growing burden, all hope is not lost. Recent therapeutic advancements, particularly the dual actions of SGLT2 inhibitors and GLP-1 receptor agonists, have shown remarkable improvements in cardiovascular and kidney outcomes. These treatments offer new hope, slowing the progression of kidney disease in people with diabetes and improving their long-term prognosis (2).
For comprehensive insights into drug treatment in renal failure, explore our database Renbase.
New therapies, like SGLT2 inhibitors and GLP-1 receptor agonists, offer hope by slowing kidney disease progression and improving outcomes.
News produced by Medbase Medical Team
References
Bello AK, Okpechi IG, Levin A, et al.; ISN-GKHA Group. An update on the global disparities in kidney disease burden and care across world countries and regions. Lancet Glob Health. 2024 Mar;12(3):e382-e395. doi: 10.1016/S2214-109X(23)00570-3. PMID: 38365413.
Apperloo EM, Neuen BL, Fletcher RA, et al. Efficacy and safety of SGLT2 inhibitors with and without glucagon-like peptide 1 receptor agonists: a SMART-C collaborative meta-analysis of randomised controlled trials. Lancet Diabetes Endocrinol. 2024 Aug;12(8):545-557. doi: 10.1016/S2213-8587(24)00155-4. Epub 2024 Jul 8. PMID: 38991584.
Tetracycline antibiotics may be used for up to three weeks also when breastfeeding
Science to practice Latest highlights on drug safety and efficacy
12.12.2024
Use of systemic tetracycline antibiotics during breastfeeding has long been of concern due to risk of dental staining of the breastfed infant associated with long-term use, such as for treatment of maternal acne. These drugs are excreted into breast milk in relatively low amounts, and, e.g. for doxycycline, it has been shown that simultaneous ingestion of milk reduces the absorption by up to 50% (1).
It appears from literature searches that substantial new information has not been published lately, but the apparent lack of reported adverse effects has led to gradual prolongation of the recommended maximal length of use from one week (2) to the current practice of 3 weeks, as also used by the Helsinki University Hospital Teratology Information Service.
Thus, as a precaution, long term (over 3 weeks) or repeated courses of tetracycline antibiotics seem best to be avoided when breastfeeding, as even low exposure levels over prolonged period of time may lead to adverse effects.
Tetracycline antibiotics can be used for up to three weeks during breast-feeding, as low milk excretion and minimal reported adverse effects have extended the recommended use.
For comprehensive insights into drug safety and efficacy during pregnancy and lactation, explore our databases Gravbase and Lactbase.
News produced by Medbase Medical Team
References
Meyer FP, Specht H, Quednow B, Walther H. Influence of milk on the bioavailability of doxycycline–new aspects. Infection. 1989 Jul-Aug;17:245-6.
Nahum GG, Uhl K, Kennedy DL. Antibiotic use in pregnancy and lactation: what is and is not known about teratogenic and toxic risks. Obstet Gynecol 2006 May;107(5):1120-38
Science to practice Latest highlights on drug safety and efficacy
18.11.2024
At least one actionable pharmacogenetic mutation is present in 97-99% of population (1,2). More than half had three or more mutations (2). Drugs that are affected by these variants had been prescribed to 31-37% of these patients (1,2), two prescriptions to 25% of patients, and three prescriptions to 12% of patients during follow-up (2).
Many commonly used drugs are pharmacogenetically sensitive. Ten most frequently prescribed drugs were simvastatin, tramadol, ondansetron, codeine, citalopram, clopidogrel, allopurinol, warfarin, amitriptyline and paroxetine (2). A substantial number of patients are exposed to drugs for which they carry potentially problematic variants leading to adverse effects or inefficacy of the drug.
Explore Medbase’s dedicated pharmacogenetic database, Pgxbase, for more information on the impact of genetic variants on drug safety and efficacy.
A substantial number of patients are exposed to drugs for which they carry potentially problematic variants leading to adverse effects or inefficacy of the drug.
News produced by Medbase Medical Team
References
Chanfreau-Coffinier C, Hull LE, Lynch JA, et al. Projected Prevalence of Actionable Pharmacogenetic Variants and Level A Drugs Prescribed Among US Veterans Health Administration Pharmacy Users. JAMA Netw Open. 2019;2(6):e195345. doi:10.1001/jamanetworkopen.2019.5345).
Hodel F, De Min MB, Thorball CW, Redin C, Vollenweider P, Girardin F, Fellay J. Prevalence of actionable pharmacogenetic variants and high-risk drug prescriptions: A Swiss hospital-based cohort study. Clin Transl Sci. 2024 Sep;17(9):e70009. doi: 10.1111/cts.70009. PMID: 39263940; PMCID: PMC11391267.
Herbal products containing ashwagandha and turmeric/curcumin linked to liver injury
Ashwagandha (Withania somnifera), often called Indian ginseng, is widely used in Ayurvedic medicine and has gained popularity in the West. Though typically well-tolerated, there have been reports of severe liver injury associated with its use, including cases of cholestatic hepatitis and elevated liver enzymes.
28.10.2024
Herb-induced liver injury (HILI) caused by herbal preparations and dietary supplements is a significant cause of acute liver dysfunction and failure (1-4). Herbal products and supplements account for approximately 16-20% of all drug-induced liver injury (DILI) cases (3,4). These liver injuries are typically caused by combination products, making it difficult to identify the specific ingredient responsible for the damage (4,5). In recent years, evidence of liver damage associated with ashwagandha and turmeric/curcumin has increased (5,6).
Ashwagandha
Ashwagandha (Withania somnifera) is a medicinal herb also known as Indian ginseng. Ashwagandha-based herbal products have been widely used in Ayurvedic medicine for the treatment of various conditions and have gained popularity in Western countries (5). Clinical studies evaluating ashwagandha have rarely reported significant adverse effects (7,8,9). However, twenty-two cases of severe liver injury linked to ashwagandha use have been reported, with causality described as definite or probable (5,6, 23,24,25). These liver injuries were typically cholestatic or mixed in nature, characterized by significant hyperbilirubinemia, severe jaundice, and itching (5,24,25). Some patients also experienced significantly elevated liver transaminase levels (5,24,25). Liver biopsies revealed mild to moderate inflammatory cholestatic hepatitis and bile duct obstruction (5). In several cases, necrosis of liver tissue associated with cholestatic hepatitis were described (6,24). Bilirubin and transaminase levels typically returned to normal within 1-9 months after discontinuation of the herbal product (5,6,24). However, one case-report described ashwagandha-associated acute liver failure requiring liver transplantation (23).
Although ashwagandha is widely used in Ayurvedic medicine and generally considered safe, twenty-two cases of severe liver injury have been reported. These injuries were typically cholestatic or mixed, with symptoms including severe jaundice, elevated liver enzymes, and, in one case, acute liver failure requiring a transplant.
Turmeric
Turmeric (Curcuma longa) is a widely used spice, and its medicinal use has increased in Western countries. Turmeric contains curcuminoids, the most significant of which is curcumin (0.6-5% dry weight; 77% of curcuminoids) (10). The European Food Safety Authority (EFSA) has set the acceptable daily intake (ADI) of curcumin at 3 mg/kg/day, which equates to approximately 210 mg per day for a 70 kg adult (11). Curcumin has low systemic absorption, and its bioavailability is limited when taken orally (12,13). Various methods have been explored to improve curcumin’s bioavailability, the most common of which is the addition of piperine (an alkaloid extracted from black pepper) to curcumin supplements (14,15). This may increase curcumin bioavailability by up to 20 times (14,15). The mechanism by which piperine enhances curcumin exposure is not fully estabished, but it may involve the inhibition of UDP-glucuronosyltransferases (UGTs) or sulfotransferases (SULTs), and potentially the inhibition of CYP enzymes at higher doses (16,17,18).
Turmeric and curcumin supplements are generally well tolerated, with significant side effects being rare, apart from mild gastrointestinal symptoms (14,19). However, liver injuries related to turmeric supplements are becoming a growing concern (19,20). At least 48 cases of liver injury, typically acute non-infectious hepatitis or mixed cholestatic hepatitis, some of which were severe, have been linked to turmeric and curcumin use (14,19,20,21). Symptoms of hepatotoxicity appeared 2 weeks to 10 months after starting the supplements, and patients showed markedly elevated transaminase and total bilirubin levels (14,19,20). Patients experienced nausea, epigastric pain, jaundice, and itching (14,19,20). In one patient, a liver biopsy revealed significant accumulation of curcuminoids in the sample (19). In most hepatotoxicity cases, the suspected turmeric/curcumin product also contained piperine (14,19). In approximately 67% of hepatotoxicity cases, the daily dose of curcumin was 1.6 to 7 times higher than EFSA’s recommended daily intake (11,14,19). It is possible that concurrent exposure to piperine further increased systemic exposure to curcumin and its metabolites (14,15,19). Additionally, high doses of piperine may themselves be hepatotoxic (14,19). The presence of the HLA-B*35:01 allele may also be a risk factor for curcumin-induced liver injury (20,21).
In most cases, liver function tests returned to normal after discontinuation of the turmeric/curcumin supplement (positive dechallenge), but three patients died (14,19,20).
Awareness of liver damage caused by dietary supplements and herbal products has increased (1,2,3,5,19,20,21,24,25). The Working Group of Heads of European Food Safety Authorities has published a list of 13 substances that it seeks to ban or restrict in dietary supplements due to potential health risks (22). Ashwagandha, curcumin (in turmeric products), and piperine are among these substances (22). It is essential for healthcare professionals to consider the hepatotoxic potential of herbal products in differential diagnoses and actively inquire about patients’ use of dietary supplements and herbal products during medical history-taking.
Learn more about ashwagandha and curcumin in the Herbalbase
News produced by Medbase Medical Team
References
Hillman L, Gottfried M, Whitsett M, Rakela J, Schilsky M, Lee WM, Ganger D. Corrigendum: Clinical Features and Outcomes of Complementary and Alternative Medicine Induced Acute Liver Failure and Injury. Am J Gastroenterol. 2016 Oct;111(10):1504.
Navarro VJ, Khan I, Björnsson E, Seeff LB, Serrano J, Hoofnagle JH. Liver injury from herbal and dietary supplements. Hepatology. 2017 Jan;65(1):363-373.
Björnsson ES, Bergmann OM, Björnsson HK, Kvaran RB, Olafsson S. Incidence, presentation, and outcomes in patients with drug-induced liver injury in the general population of Iceland. Gastroenterology. 2013 Jun;144(7):1419-25, 1425.e1-3; quiz e19-20.
Navarro VJ, Barnhart H, Bonkovsky HL, Davern T, Fontana RJ, Grant L, Reddy KR, Seeff LB, Serrano J, Sherker AH, Stolz A, Talwalkar J, Vega M, Vuppalanchi R. Liver injury from herbals and dietary supplements in the U.S. Drug-Induced Liver Injury Network. Hepatology. 2014 Oct;60(4):1399-408.
Björnsson HK, Björnsson ES, Avula B, Khan IA, Jonasson JG, Ghabril M, Hayashi PH, Navarro V. Ashwagandha-induced liver injury: A case series from Iceland and the US Drug-Induced Liver Injury Network. Liver Int. 2020 Apr;40(4):825-829.
Ireland PJ, Hardy T, Burt AD, Donnelly MC. Drug-induced hepatocellular injury due to herbal supplement ashwagandha. J R Coll Physicians Edinb. 2021 Dec;51(4):363-365.
Andrade C, Aswath A, Chaturvedi SK, Srinivasa M, Raguram R. A double-blind, placebo-controlled evaluation of the anxiolytic efficacy of an ethanolic extract of withania somnifera. Indian J Psychiatry 2000 Jul;42(3):295-301.
Cooley K, Szczurko O, Perri D, Mills EJ, Bernhardt B, Zhou Q, Seely D. Naturopathic care for anxiety: a randomized controlled trial ISRCTN78958974. PLoS One 2009 Aug 31;4(8):e6628.
Chandrasekhar K, Kapoor J, Anishetty S. A prospective, randomized double-blind, placebo-controlled study of safety and efficacy of a high-concentration full-spectrum extract of ashwagandha root in reducing stress and anxiety in adults. Indian J Psychol Med 2012 Jul;34(3):255-62.
Final assessment report on Curcuma longa L., rhizoma – Revision 1. EMA Committee on Herbal Medicinal Products. Published 24/01/2019.
EFSA Panel on Food Additives and Nutrient Sources added to Food (ANS) Scientific Opinion on the re‐evaluation of curcumin (E 100) as a food additive. EFSA Journal. 2010;8(9):1679. Available from: www.efsa.europa.eu/en/efsajournal/pub/1679.
Liu W, Zhai Y, Heng X, Che FY, Chen W, Sun D, Zhai G. Oral bioavailability of curcumin: problems and advancements. J Drug Target 2016 Sep;24(8):694-702.
Shen L, Liu CC, An CY, Ji HF. How does curcumin work with poor bioavailability? Clues from experimental and theoretical studies. Sci Rep 2016 Feb 18;6:20872.
Menniti-Ippolito F, Ippoliti I, Pastorelli AA, Altieri I, Scalise F, De Santis B, Debegnach F, Brera C, Pacifici R, Pichini S, Pellegrini M, Rotolo MC, Graziano S, Palazzino G, Multari G, Gallo FR, Neri B, Giannetti L, Russo K, Fedrizzi G, Bonan S, Mazzanti G, Moro PA, Salvi E, Firenzuoli F, Valeri A, Moretti U, Traversa G, Silano M, Stacchini P, Boniglia C. Turmeric (Curcuma longa L.) food supplements and hepatotoxicity: an integrated evaluation approach. Ann Ist Super Sanita. 2020 Oct-Dec;56(4):462-469.
Shoba G, Joy D, Joseph T, Majeed M, Rajendran R, Srinivas PS. Influence of piperine on the pharmacokinetics of curcumin in animals and human volunteers. Planta Med. 1998 May;64(4):353-6.
Zeng X, Cai D, Zeng Q, Chen Z, Zhong G, Zhuo J, Gan H, Huang X, Zhao Z, Yao N, Huang D, Zhang C, Sun D, Chen Y. Selective reduction in the expression of UGTs and SULTs, a novel mechanism by which piperine enhances the bioavailability of curcumin in rat. Biopharm Drug Dispos. 2017 Jan;38(1):3-19.
Volak LP, Ghirmai S, Cashman JR, Court MH. Curcuminoids inhibit multiple human cytochromes P450, UDP-glucuronosyltransferase, and sulfotransferase enzymes, whereas piperine is a relatively selective CYP3A4 inhibitor. Drug Metab Dispos. 2008 Aug;36(8):1594-605.
Volak LP, Hanley MJ, Masse G, Hazarika S, Harmatz JS, Badmaev V, Majeed M, Greenblatt DJ, Court MH. Effect of a herbal extract containing curcumin and piperine on midazolam, flurbiprofen and paracetamol (acetaminophen) pharmacokinetics in healthy volunteers. Br J Clin Pharmacol. 2013 Feb;75(2):450-62.
Lombardi N, Crescioli G, Maggini V, Ippoliti I, Menniti-Ippolito F, Gallo E, Brilli V, Lanzi C, Mannaioni G, Firenzuoli F, Vannacci A. Acute liver injury following turmeric use in Tuscany: An analysis of the Italian Phytovigilance database and systematic review of case reports. Br J Clin Pharmacol. 2021 Mar;87(3):741-753.
Halegoua-DeMarzio D, Navarro V, Ahmad J, Avula B, Barnhart H, Barritt AS, Bonkovsky HL, Fontana RJ, Ghabril MS, Hoofnagle JH, Khan IA, Kleiner DE, Phillips E, Stolz A, Vuppalanchi R. Liver Injury Associated with Turmeric-A Growing Problem: Ten Cases from the Drug-Induced Liver Injury Network [DILIN]. Am J Med. 2023 Feb;136(2):200-206.
Garaizabal Azkue ÍJ, Castiella A, Aburruza Ucar L, Torrente Iranzo S, Zapata Morcillo E. Turmeric associated liver injury (DILI) with susceptible HLA. Rev Esp Enferm Dig. 2024 Sep 19;
Working Group Food Supplements of Heads of Food Safety Agencies: First report of the HoA Working Group “Food Supplements” (2024).
Suryawanshi G, Abdallah M, Thomson M, Desai N, Chauhan A, Lim N. Ashwagandha-Associated Acute Liver Failure Requiring Liver Transplantation. Am J Ther. 2023 Jan-Feb 01;30(1):e80-e83.
Philips CA, Valsan A, Theruvath AH, Ravindran R, Oommen TT, Rajesh S, Bishnu S, Augustine P. Ashwagandha-induced liver injury-A case series from India and literature review. Hepatol Commun. 2023 Oct 1;7(10).
Koturbash I, Yeager RP, Mitchell CA, Ferguson S, Navarro VJ, Paine MF, Roe AL. Botanical-induced toxicity: Liver injury and botanical-drug interactions. A report on a society of Toxicology Annual Meeting symposium. Regul Toxicol Pharmacol. 2024 Sep 19;153:105708.